
Acoustic Neuroma
Vestibular schwannomas - commonly called by the misnomer, acoustic neuroma - are benign growths arising from the balance nerve. Because they are benign, the do not metastasize, or spread to other parts of the body. They are uncommon, and occur in approximately 10 people per million per year in the United States. They tend to be found in patients older than 40 years.
The vast majority (95%) of these tumors are sporadic, meaning they are not passed on through genes. Sporadic tumors occur in only one ear, and there are no known risk factors. Rarely these tumors are associated with a genetic disease called Neurofibromatosis Type II. Patients with Neurofibromatosis develop tumors at a younger age, usually have tumors on both sides and also have other manifestations, including benign tumors of the brain and dura (the covering of the brain).
Vestibular schwannomas are generally slow growing (less than 3 millimeters per year) and may not grow at all if followed over time. However, tumor growth is not predictable, and some tumors grow more rapidly. When tumors are small they may give no symptoms or very subtle symptoms, such as a slight hearing loss or a noise in the ear (tinnitus). When tumors grow, they begin to cause injury to the hearing nerve and balance nerve, by compressing them. Patients may experience severe hearing loss (either suddenly or progressively over a period of years) or balance problems. Large tumors may compress the brainstem and result in headaches and other symptoms of increased intracranial pressure. Symptoms don’t correlate well with size. Some patients with very small tumors may have obvious symptoms and likewise, some patients with large tumors may have no symptoms at all.
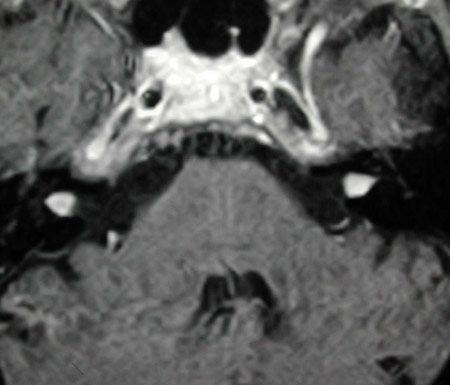
The diagnosis of vestibular schwannoma is made by history, hearing tests, and MRI scan. Gadolinium is a special contrast agent used during the MRI to allow visualization of the tumors. With good technique, MRI will show tumors as small as 2-4 millimeters.

MRI showing 2mm vestibular schwannoma in right internal auditory canal.
MRI showing bilateral vestibular schwannomas
HOW IS A VESTIBULAR SCHWANNOMA TREATED?
The goal of treatment for benign tumors is to eradicate the tumor while preserving form and function. This holds true for vestibular schwannomas as well. There are three treatment options for patients with a vestibular schwannoma, observation, radiotherapy, and surgery. Which option is best for each individual must be carefully determined based on the size of the tumor, the location of the tumor, the symptoms, the patient’s age and general health, and the patient’s goals and concerns. This decision is made by the patient after discussing all the options, each with unique risks and benefits.
OBSERVATION OR “WATCHFUL WAITING”
Observation entails exactly that. The patient is observed for hearing, balance, tinnitus, and facial nerve function. An MRI is performed yearly or every 6 months depending on the rate of tumor growth. This approach is ideal for a patient with a small, non-growing tumor, without dizziness, who is older and whose health precludes surgery.
Advantages
- May avoid surgery
- May avoid radiation
Disadvantages
- Tumor is still there and does not disappear
- MRI must be done at least once every 1-2 years
- Hearing loss and dizziness may develop or worsen, even if the tumor is not growing
- May be more difficult to perform hearing preservation surgery later only if the tumor grows, treatment will be needed
- May be more difficult to preserve normal facial function if tumor has grown or become attached to facial nerve
RADIOTHERAPY
Stereotactic radiation therapy (commonly called, radiosurgery) is a term used to describe several specific radiation techniques including Gamma Knife Surgery, LINAC, and fractionated radiosurgery, depending on the type of radiation beam and type of machinery used . Stereotactic radiotherapy is a method of delivering a radiation dose in such a way as to minimize the dose of radiation to surrounding normal tissues (brain) while delivering a very high dose to the tumor. Low dose beams of radiation are aimed from many different directions by a computer to focus on the tumor. This is performed in a single session without anesthesia requiring only a 1-2 day hospital stay. Radiotherapy is attractive to many patients because of the short-term low complication rates and a shorter hospital stay. This form of treatment is not appropriate for a patient with a tumor larger than 3cm in diameter, as radiosurgery is ineffective in larger tumors.
Advantages
- Good control rate for small tumors (>90%) with less than 5 years followup
- Avoid surgery
- Short stay in hospital
- Quick recovery
Disadvantages
- Tumor is still present and tumor cells are alive
- Tumor may grow and require surgery as late as 10 years or more after radiation
- Surgery for a growing tumor after radiation is more difficult and risks are greater
- MRI must be done every year
- Delayed facial numbness, facial paralysis, balance problems and hearing loss, all generally irreversible
- Remote risk of transformation of benign tumor into a cancer
- Long term (10year) results and risks are not clear
- SURGERY
The choice of surgical approach depends on the size and location of the tumor and the degree of hearing loss. In some cases, it is possible to save hearing. With larger tumors, hearing must be sacrificed in order to successfully remove all of the tumor. Total removal of the tumor without complications is the surgical goal. Occasionally, partial removal is done. This is sometimes desired in order to save facial nerve function. Surgery is performed under general anesthesia and requires a 4-6 day hospital stay. During surgery, a computer is used to monitor the facial nerve and the hearing nerve.
Advantages
- Tumor is completely removed and risk of recurrence is remote (<0.1%)
- Only one follow-up MRI is needed
- If hearing is preserved, it is stable over time
- Minimal long term side effects
Disadvantages
- Intracranial surgery with inherent risks
- General anesthesia
- 4-6 day hospital stay
- Risk of short term facial paralysis and balance problems
- In some cases, hearing cannot be saved
- Recovery period of 4-6 weeks to regain strength and balance
SURGICAL APPROACHES
Translabyrinthine approach
This involves an incision behind the ear. The mastoid and inner ear structures are removed by a drill to allow exposure of the tumor. The facial nerve is identified in a segment unaffected by tumor prior to tumor dissection in order to protect it during tumor dissection. Exposure to the tumor is the widest with this approach. The entire tumor is visualized and removed. The mastoid defect is filled with fat removed from the belly and often covered with a titanium plate.
With this approach, hearing and balance function on the tumor side are sacrificed. The affected ear is permanently deaf. Patients compensate well for the hearing loss, but some wish for a bone anchored hearing aid or CROS hearing aid to help in difficult situations. Balance function recovers to normal or near-normal within a few weeks. This approach offers the best facial nerve exposure and protection.
Middle Fossa approach
An incision is made above the ear, and a window of bone is temporarily removed from the side of the skull. By elevating the brain and dura away from the bone and removing by drill bone overlying the inner ear, the tumor is approached from above. Here, the inner ear is saved. Again the facial nerve is identified in a normal segment prior to tumor dissection. This approach provides very good exposure of small tumors in the bony internal auditory canal, but less exposure to larger tumors which reach the brainstem. After the tumor is removed, the brain is released, fat is used to patch the defect left by the tumor, and the skull is repaired.
Hearing can be preserved in 60-70% of these surgeries. In some cases, the tumor involves the hearing nerve and requires sacrifice. In other cases, even though the tumor was entirely removed without obvious injury to the hearing nerve, hearing may be lost. The reason for this loss is not clear, but most likely is a result of the loss of microscopic blood supply to the hearing nerve.
Retrosigmoid approach
An incision is made far behind the ear for this approach. The dura is opened and the brain is elevated to expose the tumor at the level of the brainstem. The tumor is debulked in order to visualize the facial and hearing nerves. Then, the bone is drilled away from the skull adjacent to the nerves to expose more of the nerves and tumor in the internal auditory canal. After this the remaining tumor is removed. The defect is closed by repairing the dura and the skull defect.
In about 50-70% of cases, hearing may be preserved, even with larger tumors. One disadvantage of this approach is a restriction of exposure to the far end of the tumor risking an incomplete resection. In some cases, hearing is lost despite having protected the hearing nerve during dissection, possibly because of loss of microscopic blood supply to the nerve.