
Cochlear Implant
Cochlear implantation is a life-changing event to many patients with hearing losses that are not effectively managed with well-fit hearing aids. With the experience most implant users are able to understand spoken speech in the everyday world. Some patients are able to enjoy music and/or hold conversations on the phone. The implant does not restore normal hearing, and many patients describe its sound as mechanical. However, with time and practice, the brain adapts to the new “sound” and speech signals and environmental sounds begin to sound more natural. The primary benefits of a cochlear implant are: (1) aid in lip reading; (2) perception of environment sounds; (3) aid in monitoring the volume of one’s own voice.
The ideal candidates for cochlear implantation are adults or children with recent hearing loss and young children whose hearing loss is identified very early. People with prior hearing experience adjust very well and often very quickly to hearing with a cochlear implant. They report significant satisfaction and improved quality of life. Deaf children implanted before the age of 5 also do very well. With time and rehabilitation, they develop very good speech understanding as well as speech production skills. The majority of these children are able to attend mainstream schools. Children who are implanted before the age of 2 seem to do even better than those implanted between 2 and 5 years old.
For adults and teens who have been deaf for most of their lives, were educated with manual language, and live in the deaf community, cochlear implantation has been very controversial. Not only are there medical issues, but more importantly social issues. Fortunately, the strong opposition to implantation from the deaf community is lessening. More and more prelingually deafened and long term deafened patients are seeking information on cochlear implants. For those people who are good lip-readers, who have some spoken language skills, and who are committed to learning and adapting to the use of the implant, cochlear implantation may provide significant benefit. Users like this report better communication with hearing family and friends, better use of environmental sounds, and improvement in quality of life.
This technology is continuing to improve thanks to the work of many scientists throughout the world. Current research includes improvement of speech processing technology, improving performance by implanting bilateral devices and preserving residual hearing, expanding the eligibility requirements by looking at patients with more residual hearing and prelingual deafness, improving the design of the device to one day be 100% implantable, and improving the function of the inner ear by preventing injury to the sensitive inner ear structures with new medications and potentially gene therapy.
WHAT IS A COCHLEAR IMPLANT?
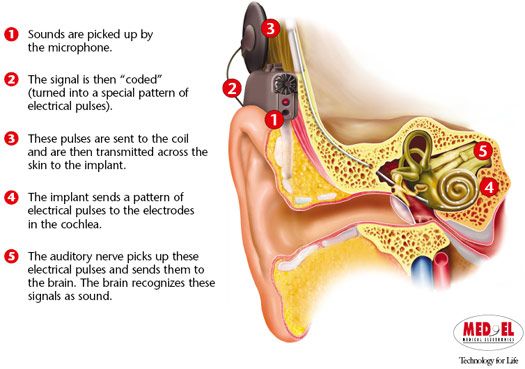
A cochlear implant is a device that provides sound perception through direct electrical stimulation of the hearing nerve, bypassing the inner ear – the most common culprit of hearing loss. A cochlear implant is comprised of two parts – and internal device and an external device. The internal device is surgically implanted under the skin and is comprised of a receiver, a magnet, and a bundle of fine wires, the electrode array. The external device includes the sound processor, a cable and a microphone - all housed in an earpiece. The sound processor analyzes incoming sounds from the microphone and converts those sounds into patterns of electrical current. The current is carried along the cable and delivered across the skin by radio wave transmission to a receiver implanted under skin. The receiver carries the current to the electrode array which has been implanted into the cochlea, the portion of the inner ear that contains hearing nerve fibers. The current stimulates fibers of the auditory nerve and results in the perception of sound.
WHO BENEFITS FROM A COCHLEAR IMPLANT?
Cochlear implants can help patients with severe to profound sensorineural hearing loss in both ears who cannot benefit adequately from the use of hearing aids. People of all ages can qualify, from age 1-100. The ideal candidate has hearing loss of short duration. In children born with deafness, early implantation is preferred, so that they may experience speech sounds in time to begin learning language before the age of 2-3. In special cases, implantation may be performed on patients with long-term deafness.
WHAT KINDS OF HEARING LOSSES ARE TREATED WITH A COCHLEAR IMPLANT?
The cochlear implant is designed for patients with sensorineural hearing loss that have failed conventional treatment including medications and hearing aids. Sensorineural hearing loss is a specific type of hearing loss, defined as any abnormality of the inner ear or auditory nerve that prevents transfer of electrical signals to the auditory nucleus (the brain’s center for hearing).
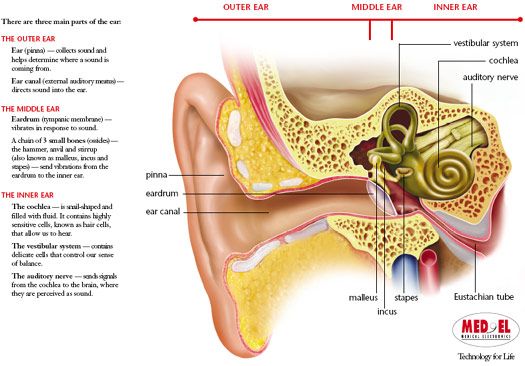
Normally, when sound vibrations enter the ear canal, they are collected by ear drum, conducted through the middle ear by three small bones (ossicles), and converted to pressure waves in the fluid of the cochlea (snail shaped structure of the inner ear). These pressure waves travel through the inner ear fluid and result in motion of the fibers at the top of the inner ear hair cells. The motion of the fibers activates the hair cells and result in an electrical signal. This signal is carried along the auditory nerve to the brain.
In many cases of sensorineural hearing loss, the problem is due to hair cell damage. However, a significant number of auditory nerve fibers are still functional. Since the cochlear implant sends an electrical signal that stimulates the nerve fibers directly, bypassing the inner ear, these patients may perceive sound with the implant despite the damage in the inner ear.
CAN EVERY PATIENT WITH SEVERE TO PROFOUND SENSORINEURAL HEARING LOSS BENEFIT FROM A COCHLEAR IMPLANT?
Many people of all ages with many different kinds and patterns of hearing loss can qualify for cochlear implantation.
Unfortunately, not everyone can benefit from using a cochlear implant. Some forms of sensorineural hearing loss are a result of destruction of or absence of the auditory nerve fibers. Therefore, there is nothing for cochlear implant to stimulate. In other forms of hearing loss, structural abnormalities of the inner ear prevent surgical implantation. In many forms of sensorineural deafness, the status of the auditory nerve fibers is unknown. In such cases, it can be difficult to predict the potential benefit of receiving a cochlear implant. Currently, researchers are studying the role of auditory nerve fiber survival to better predict performance before implantation. The duration of hearing loss and the age at which it occurred also seem to influence performance with an implant.
HOW DO I KNOW IF I AM A CANDIDATE?
Candidacy for cochlear implantation is determined by a team of specialists which includes an Otologist (ear doctor), an audiologist, a speech therapist, an educational specialist, a social worker, and a psychologist. The Otologist will obtain a complete history, perform a thorough exam, and order appropriate testing. The audiologist will evaluate your hearing by performing an audiogram (hearing test) and will also determine the appropriateness of amplification use. Other team members will also meet with and perform evaluations when necessary. A review board then will evaluate this information to determine whether you are cochlear implant candidate.
WHAT IS INVOLVED IN HAVING A COCHLEAR IMPLANT OPERATION?
Cochlear implantation surgery is performed under general anesthesia and takes approximately one-two hours. An incision is made behind the ear and operating with the aid of a microscope, the surgeon drills away a portion of the mastoid bone (hard bone behind the ear) to gain access to the inner ear. A small opening is created into the cochlear. The electrode array is threaded into the cochlea and its outer end is attached to the bone of the skull. The incision is closed and the head bandaged. Most patients go home the next morning. Patients return the following week for suture removal.
WHEN CAN I BEGIN USING THE IMPLANT?
The patient returns at approximately one month following surgery to begin using the sound processor. The processor “hook-up” and programming is performed by the audiologist. The initial programming takes several hours. During this visit the audiologist and patient design a “MAP”. This MAP is the set of parameters of electrode stimulation that give the patient the best hearing. In the subsequent few months, there are a series of visits to the audiologist to test and adjust the signal levels for the electrodes in the array. These settings can be updated at each visit over a period of weeks or months, as the patient becomes more comfortable with experiencing sound again. At first, sounds may be quite different than remembered prior to the hearing loss. Environmental sounds are usually the first to be identified or relearned. With training and experience, the patient’s perception of speech improves.
ARE THERE ANY ALTERNATIVES TO A COCHLEAR IMPLANT?
Currently, cochlear implantation is limited to patients who cannot benefit significantly from using conventional hearing aids and other hearing assistive devices. Use of some combination of lip reading, cued speech, sign language, and powerful hearing aids are alternatives to implant surgery. An audiologist can direct you to sources for counseling and assistance that emphasize these alternatives.
WHAT ARE THE BENEFITS OF THE COCHLEAR IMPLANT?
The improvement in auditory perception (hearing) following cochlear implantation varies widely from patient to patient. Nearly all patients have some perception of sound. Even if this awareness is only the detection of the presence of absence of a sound in the environment, it can be substantial aid to lip-reading. In most cases, implantees have some additional ability to discriminate pitch and loudness, which further enhances the benefit of the device. In some patients, the implant may even provide enough hearing to understand speech without lip-reading, to permit use of the telephone and to enjoyment of music.
WHAT ARE THE RISKS OF COCHLEAR IMPLANTATION?
Risks associated with cochlear implantation include those associated with the surgery itself, such as bleeding, infection, problems with anesthesia or healing, dizziness, or injury to the facial nerve. In addition, there are risks associated with the implant, such as mechanical or electrical failure, rejection, infection and problems what would require removal or replacement of the implant. Your surgeon will discuss all of these risks with you. Usually any and all hearing present in the operative ear prior to surgery will be completely lost at time of implant surgery. New techniques and devices are being developed with the goal of preserving residual hearing.
COCHLEAR IMPLANTATION AND MENINGITIS
Recently a possible link between cochlear implantation and meningitis has been suggested. The Center for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA) and others published a study addressing this issue in the July 31, 2003 issue of The New England Journal of Medicine. In 4264 children implanted before age six, they found an incidence of meningitis of just over one half of one percent (0.6% or 26 patients). The authors reported that: 1) Meningitis occurred more often in children with cochlear implants than in children of the same age group in the general population. 2) Children who received a cochlear implant with a positioner were more likely to get bacterial meningitis than children with other types of cochlear implants. 3) Children with a cochlear implant who had congenital inner ear malformations alone or in association with cerebrospinal fluid leaks were at increased risk for bacterial meningitis.
Although this study is vitally important, there is one major weakness. The study infers that children with implants are at a 30 fold increased risk of meningitis compared to a normal child. This is misleading. Hearing-impaired children are at increased risk of meningitis, even without implants. In the New England article, 11.5 percent of the implanted children had an inner ear deformity that put them at risk for meningitis, with or without an implant. 23 percent of the implanted children in the study had meningitis BEFORE receiving their cochlear implant. In another report of a child who developed meningitis after a cochlear implant, the non-implanted ear was found to be the source of the infection. The implant and the implanted ear were in no way involved.
Based on this and other studies, The CDC and FDA recommend that children and adults with cochlear implants should be vaccinated for pneumococcus and children should also be vaccinated for H. Influenza. Otitis media should be treated aggressively with antibiotics and/or ventilation tubes.